MedAxiom Blog
Tuesday, March 14, 2017 | Joel Sauer

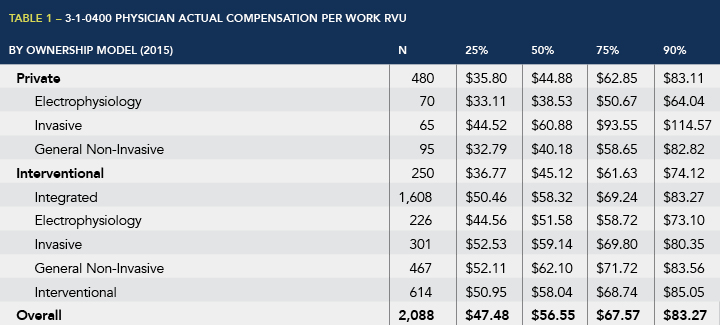
Peer surveys, like the MedAxiom Cardiovascular Provider Compensation and Production Survey, annually publish a measure showing compensation per work Relative Value Unit (wRVU). Table 1 below shows data from the most recent MedAxiom report for cardiology. This statistic is perhaps the most misunderstood of the published compensation data and, as a result, is often misused in contract negotiations.
Let’s start with a definition. What is the Physician Actual Compensation per Work RVU? Simply put, this metric is the product of total actual physician compensation divided by wRVU production. In other words, it’s a calculated rate. Each of these calculated amounts is then compared to all the others to arrive at bell curve distribution (median, 25th percentile, 75th percentile, etc.). Most surveys, including MedAxiom’s, consider compensation from all sources for the “Physician Actual Compensation.” Looking again at Table 1, the data show that the median – half of physicians earned more, half of physicians earned less – was $56 per wRVU.
So let’s use an example to make sure this very clear. If in 2015, Dr. Jones earned $515,000 from all sources (clinical comp, incentives, directorships, administrative time, etc.) and produced 8,500 wRVUs in that same time period, her compensation per wRVU calculates to $60.59 ($515,000 / 8,500). Based on the data from Table 1 (and more specifically within MedAxiom’s MedAxcess database), she would be around the 65th percentile nationally for compensation per wRVU.
However, this does not mean that Dr. Jones, who happens to be employed by a health system, was contractually paid $61 per wRVU for her production. She may in fact have an employment agreement that includes multiple income sources. Table 2 below shows an example of how this might look from a math standpoint. In fact, Dr. Jones’ employment contract specifies that she is paid $55 for each clinical wRVU she performs. In addition she is eligible for a value incentive (quality, cost, service) and performs a medical directorship and is compensated for that time. This then pushes her overall compensation per wRVU to $60.59. It is this latter number, not her contracted rate, which is published in the survey.

There’s also the notion that the published median ($56.55 in Table 1) is really what most physicians are being paid per wRVU. As can be seen in Figure 1, there is huge variability in this calculated rate, ranging from $17 per wRVU all the way up to $200. How can this be?

Consider a physician hired to work predominantly in a heart failure clinic environment. For the most part this doctor will bill within the Evaluation and Management (E&M) spectrum of the CPT codes – not a wRVU-intense ecosystem. In order to be market competitive, this organization contracted him at $550,000 per year and he was able to generate 4,500 wRVUs in the deeply subspecialized heart failure domain. This calculates out to $122 per wRVU in compensation.
However, in this same practice there is a non-invasive physician who has been predominantly assigned by the group to read imaging studies. She is also paid a base of $550,000, but is able to generate nearly 20,000 wRVUs because of the type of work performed. Her compensation per wRVU calculates out at $27.50.
Clearly I’m using extreme examples to illustrate the point, but these scenarios do exist and – when considered with other variabilities – force us to pause when putting too much weight on the compensation rate per wRVU.
How physicians in a group decide to split compensation also has a significant impact on the resulting calculated compensation per wRVU. Table 3 below shows an example of this in an integrated group who are all contractually paid $60 per wRVU, which generates a pool that the cardiologists then determine (with appropriate oversight) how to distribute individually. This group has chosen to split compensation 50 percent equally and 50 percent based on individual wRVU production – a very common phenomenon in cardiology practices. As this figure shows, there is wide variability on compensation per wRVU at the individual physician level even though contractually all are paid a consistent rate. This same example can cause widespread variability on compensation per wRVU in private groups as well.

Here are some other interesting data. When you look at the top performers in terms of generating wRVUs, there is a direct correlation with these physicians also being top total earners (top box of Table 4). However, these same top producers are in the bottom of the heap in terms of compensation per wRVU (last column of that same box). In other words, there’s an inverse relationship between high wRVU production and compensation per wRVU. Not surprisingly at all then, in this same data we find that the lowest producers in terms of wRVUs are also the lowest earners (Table 4).

Note too that in the second box of Table 4 where we sort by Total Compensation (the independent variable) that the top earners are also the highest in terms of compensation per wRVU. However, this correlation is not nearly as strong as with the comparison above. Further, you can see that correlation between being in the top earning quartile and top production in terms of wRVUs is very strong. Last, in the bottom box of Table 4 when sorting on the calculated compensation per wRVU, the correlation with Total Comp is even weaker and the inverse relationship with production remains.
Thus it is safe to conclude with cardiovascular physicians that high productivity (as compared to peers) leads to high compensation, whereas high compensation does not also mean high compensation per wRVU.
This statistic is perhaps the most misunderstood of the published compensation data and, as a result, is often misused in contract negotiations.
So in summary, the compensation per wRVU is a calculated rate, and both wRVUs and total compensation are reported; there is wide variability within the cardiovascular workforce on this measure. Further, myriad circumstances impact the resulting individual physician compensation per wRVU, including clinical role, internal distribution method, contract terms and on and on. It is extremely important for all these variables to be considered – both by administrators and physicians – when using this singular point from survey data to set physician compensation plans and for fair market testing purposes (on which I am not qualified to comment).
Not understanding what this measure is and isn’t can lead to bad conclusions.
Leave a Comment